

The opioid crisis is an objectively very difficult problem
The opioid crisis is an objectively very difficult problem
Enter the no-solutions zone

Back in 1997, the Dandy Warhols released the excellent song “Not If You Were The Last Junkie on Earth,” proclaiming that “heroin is so passé,” a sly reference to the fading heroin-chic aesthetic of the early 1990s.
Twenty-five years later, it’s clear that that forecast was badly wrong. The United States now has more people using heroin than ever, to say nothing of fentanyl, a synthetic opioid that is both easier to covertly produce and traffic than heroin and more likely to lead to overdoses.
I’ve been struggling for a while to frame my thoughts on this issue. A good post on the opioid crisis would, in theory, involve explaining how to solve the opioid crisis. To save you some time: I do not have any great ideas for how to solve the opioid crisis. But after reading a lot about this and chatting with folks who are knowledgeable, I think we need more honesty about that lack of solutions. One of the best pieces on the crisis is a 2018 article by Dan Vergano in Buzzfeed arguing that “The Opioid Crisis is Not a Metaphor.”
I think this is correct. The opioid crisis is an extremely difficult policy problem. And precisely because there isn’t an obvious policy solution, a lot of people are trying to wield the tragedy as a club to win some other argument about progressive prosecutors or trade policy or campaign finance.
But this is a problem with discrete roots in past prescription drug policy errors that we can’t simply undo. It’s gotten worse because of underlying technological changes that we also can’t undo. And a lot of the most obvious remedies (more treatment! copy Portugal!) are very hard to implement because of the broader structural features of American healthcare and criminal justice policy.
We need to try to see things as they are, not just yell at each other.
Really quick history in case you don’t know
Because no one really knows how to solve the problem, the best writing on the subject — the recent Stanford/Lancet report, German Lopez’s recent column, Patrick Radden Keefe’s “Empire of Pain,” and Sam Quinones’ “Dreamland” — dwells on the history of the opioid crisis. I recommend taking a look if you’re interested in a deep dive, but to briefly review:
Chronic pain is a difficult medical problem that causes an enormous amount of suffering. Doctors have not had a lot of success treating it.
Opioids are highly effective at reducing pain, but also highly addictive. Traditionally they were seen as suitable for acute pain (surgical recovery) or compassionate care for the terminally ill (late-stage cancer patients), but not for chronic pain where the addiction risk is too high.
Purdue Pharmaceutical introduced OxyContin in the 1990s, claiming it had features that made it abuse-resistant and thus safe to use as a chronic pain solution.
Other pharmaceutical companies introduced competing projects, and patient advocacy groups (often with an assist from Pharma dollars) invested in convincing doctors and public health agencies to give out more opioids more widely.
The safety claims were mostly false, and many OxyContin users became addicted and/or started abusing the pills.
Some unscrupulous doctors operated “pill mills” that put more drugs into circulation.
Heroin traffickers, who had traditionally served urban markets, saw an opportunity to expand into a much wider set of communities that were full of people desperate to obtain pain pills. The heroin dealers could offer a product that was cheaper and featured a more intense high.
Fentanyl is more potent than heroin per gram and has increasingly piggybacked on the heroin supply chain. Because you don’t need as much fentanyl, it is harder to interdict and also easier to overdose.
Long story short, the FDA (like the Dandy Warhols) badly misjudged the situation.
The epidemic transcends space and time
While the opioid epidemic has generated a lot of good writing on its history, it’s also prompted a lot of bad takes.
Typically, these takes involve someone linking something they’re annoyed about to the fact that lots of people are dying of opioids, often without checking to see if the numbers actually support their narrative. For example, Tucker Carlson said recently that the Biden administration is ignoring the rising death toll of opioids because it impacts white people. Democrats don’t care about white people, so they don’t care about opioids.
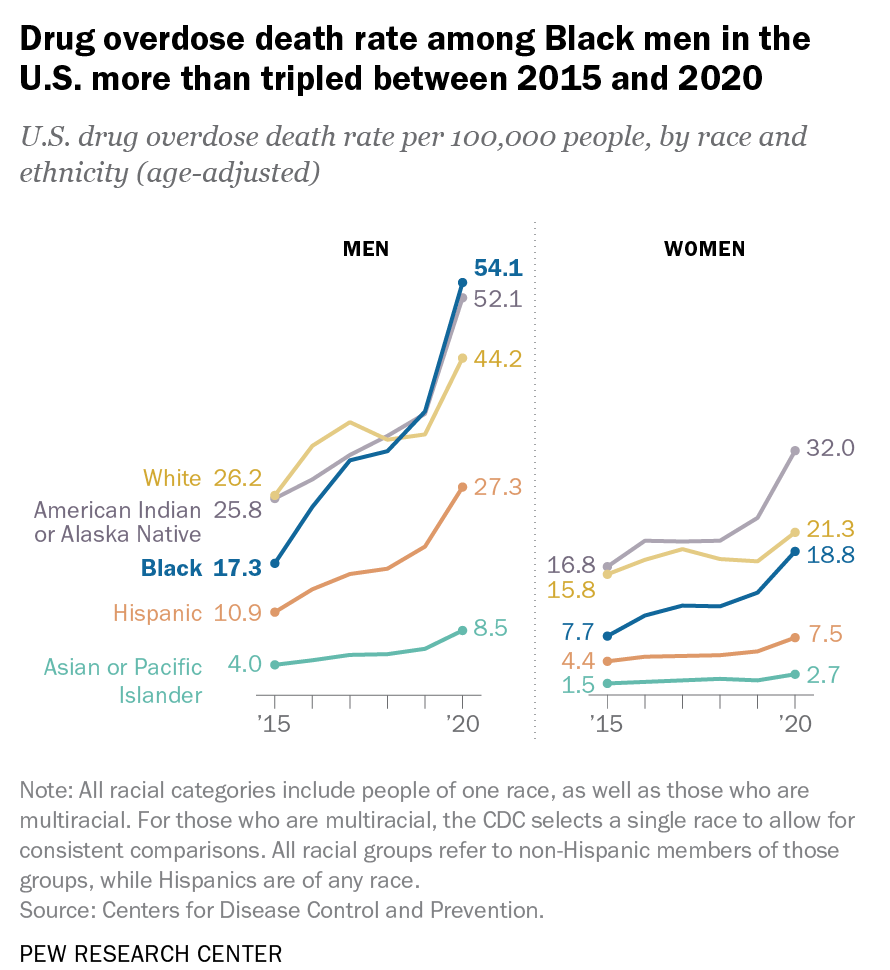
This, however, is not true. For a long time the opioid addiction crisis was disproportionately located in white communities (an ironic consequence of a well-documented pattern of racial discrimination in pain diagnosis), but the past few years have seen a surge in Black heroic and fentanyl overdoses, and the overdose death rate for Black men now exceeds that for white men.1 Biden hasn’t failed to reduce drug overdose deaths because he hates white people. He’s failed for the same reason that Trump, Obama, and Bush failed: he doesn’t know how.
By the same token, Anne Case and Angus Deaton have spun their “deaths of despair” narrative largely out of the opioid crisis. This thesis got a lot of attention circa 2015 because it aligned with widespread criticisms about the weak labor market and the impact of trade with China. The fact that, at the time, the deaths were concentrated among non-college whites also suggested interesting links to Trump’s political appeal. But we’ve learned over the past six years that Black and Latin people are not mysteriously immune to opioid addiction. In 2021, the Hispanic overdose death rate for men — though far lower than the Black or white rate that year — was actually higher than the 2015 rate for non-Hispanic whites.
Michael Shellenberger and other Bay Area critics of Chesa Boudin argue that bad progressive policy is responsible for drug addiction, and drug addiction is responsible for San Francisco’s homelessness problem. I think this is pretty clearly mistaken. The drug problem is at its most severe in places like West Virginia and Ohio where progressives aren’t in charge and where homelessness isn’t a big problem because housing is cheap.
What’s true, I think, is that drug addiction causes crime and that unhoused drug addicts are a public nuisance in a way that unhoused people who don’t suffer from addictions are not. I am generally sympathetic to the view that the soft on crime approach to managing these issues is wrong. But it’s still important to get the causal direction right, and there are just not that many progressive prosecutors in America. You cannot look at this in a fair-minded way and decide it’s Chesa Boudin’s fault.
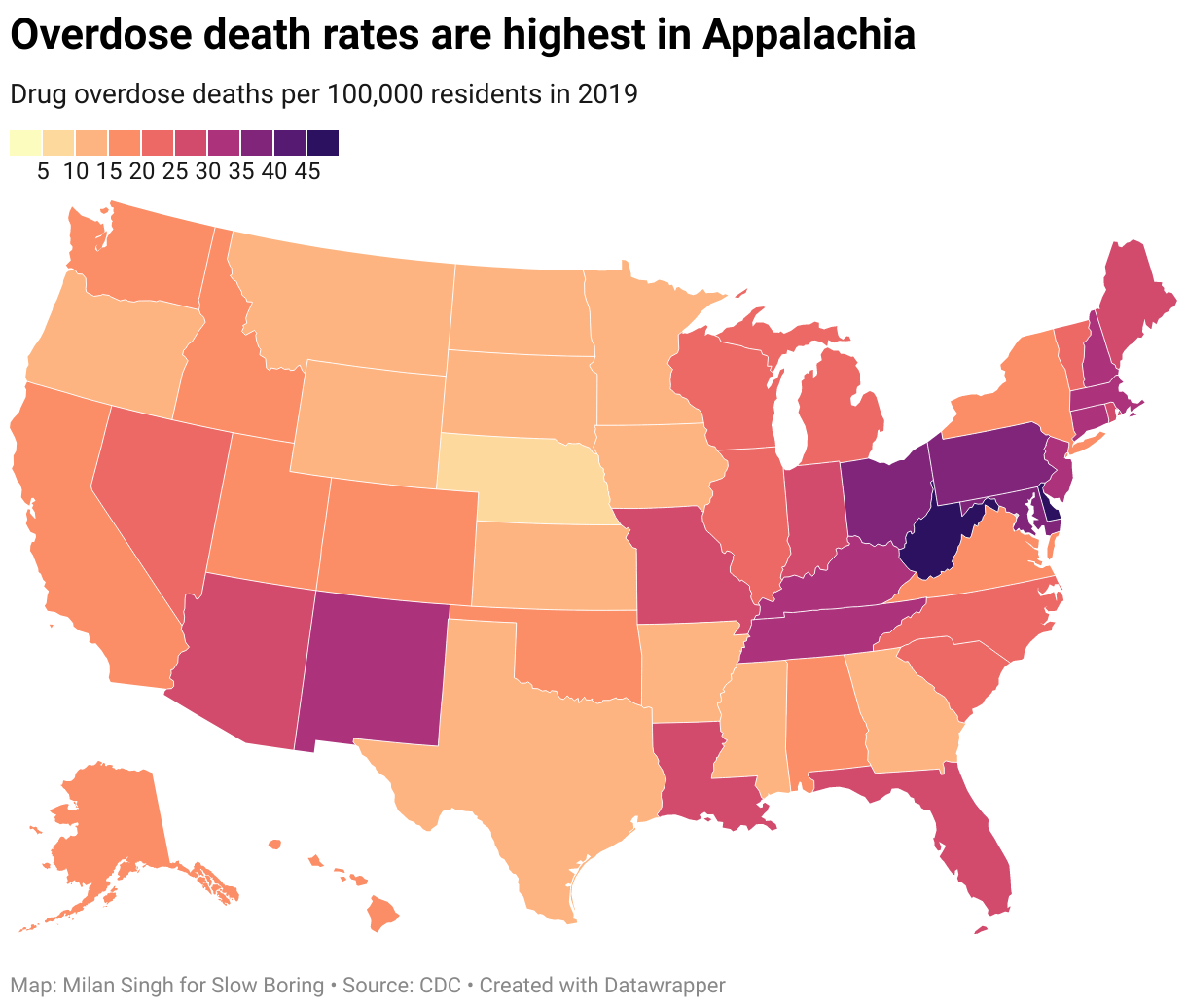
But even though the concentration in Appalachia does suggest some vaguely Case-Deaton-y conclusions, the rest of the regional pattern does not. Massachusetts and Connecticut are not experiencing industrial decline driven by trade with China; they lost their manufacturing jobs to low-wage competition from the South a generation earlier. Maryland is the richest state in the union.
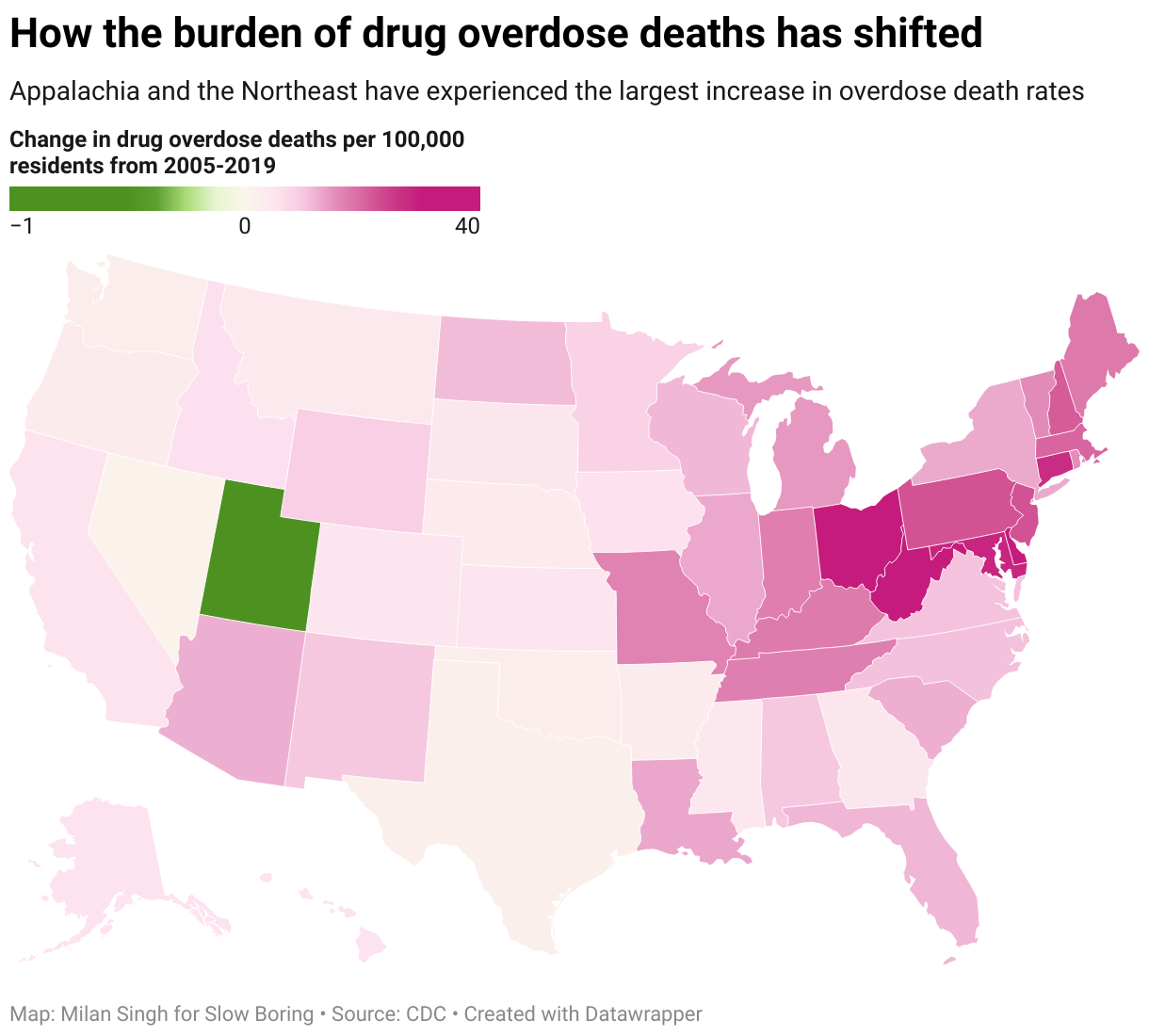
The problem is bigger than pat narratives, and it’s getting worse almost everywhere.
And the reason it keeps getting worse is that nobody’s ideas for stopping it are very good.
Fentanyl is an objectively hard problem
A perennial favorite solution to any drug problem is to try to cut off the supply. This has never worked especially well, as the first 40 years of the “war on drugs” can attest.
But it’s not as ineffective as drug war critics sometimes suppose. As the late Mark Kleiman liked to point out, marijuana is much more expensive than mass market tea or some random dried herbs at the supermarket. And that’s not because of any unique properties of the plant. The illicit status of cannabis means you cannot operate a highly efficient marijuana farm, and even the recent legalization victories in the United States haven’t really changed that.
Similarly, it’s hard to grow big fields of poppies undetected. That’s why the world ended up turning to Afghanistan for so much of its supply, which in turn led to long and difficult supply routes. So supply-side measures have had a real impact on the availability of some drugs, including heroin.
But the rise of synthetic opioids has provided a powerful workaround.
Fentanyl is made in relatively small indoor labs that are easier to conceal than large agricultural plots. And because the fentanyl itself is so potent, it can be smuggled in much smaller quantities which are hard to detect and interdict. This Quinones piece on fentanyl has some rhetorical flourishes that I wouldn’t endorse, but it captures what is basically a large positive shock to the productivity of the opioid sector of the economy driven by technological innovation. We are even seeing an economic crisis in poppy-growing regions of Mexico because traditional plant-based heroin simply can’t compete with more efficient synthetics.
When conservative publications like The New York Post run demagogic attacks on liberal harm-reduction strategies, they don’t actually offer any particularly interesting ideas for how to get tough. Some state legislatures have already passed legislation increasing prison time for convicted fentanyl traffickers and more bills are floating around in others and in Congress. The prison population will likely rise as a result, but long prison sentences for crimes you can probably get away with are a poor substitute for actually increasing the odds of detection. Incapacitation of drug dealers is not very effective; it creates a market opportunity for new drug dealers. Deterrence can work, but deterrence purely through harsher penalties is very costly and relatively ineffective.
The limits of harm reduction
Progressives prefer a harm reduction approach toward drug users.
This includes safe injection sites where no one is arrested for using, where anti-overdose drugs are available, and where users can test their drugs to make sure they’re not tainted. And I think if the number of people dealing with addiction in the U.S. was falling, harm reduction would be an easier sell.
The problem with harm reduction in the context of rising levels of addiction is twofold. One is that while people don’t like to see people die of drug overdoses, they also don’t like to see their own towns full of drug addicts committing petty crimes to support their habit. Harm reduction is, deliberately, an effort to address the public health aspect of addiction; not dead is a much better outcome than dead. But (and this is where I think Shellenberger is right), there are plenty of other problems associated with drug addiction that citizens do want to see addressed.
Right now, many places have rising numbers of addicts, rising levels of shootings, and apparently rising levels of shoplifting. As long as all that other stuff is getting worse, it’s hard to argue that harm reduction is the solution when it only even purports to address a small share of the harms.
Most of all, the impact of harm reduction measures on addiction levels is still unclear. Scholars I know and like who look at one specific aspect of this disagree. Jennifer Doleac with Anita Mukherjee finds that making anti-overdose drugs more widely available increases rates of opioid use. Richard Frank, Keith Humphreys, and Harold Pollack say that’s not the case. I think it’s hard to tell who’s right. Since that fight went down in 2018, I wish we’d gotten updates in 2019, 2020, and 2021 as more data became available. But redoing previous work isn’t generally rewarded in academia, so it’s still unclear.
But the underlying rate of addiction is, in fact, going up. And even if overdose deaths are the easiest metric by which to track the toll of the epidemic, what we want is to have fewer addicts — not just a smaller share of a growing number of addicts — dying.
You can’t put the toothpaste back in the tube
One reason we can be reasonably confident the opioid epidemic is a result of bad prescription drug policy and not postmodern ennui is that the problem hasn’t really arisen in Europe.
The United States has an unusually entrepreneurial pharmaceutical sector with more advertising, more aggressive marketing, and fewer price controls. The upside to this is that it stimulates more pharmaceutical innovation. The downside is incredibly aggressive sales of OxyContin that took a really long time to clamp down on. One of the best points made by the Stanford/Lancet Commission is that we really don’t want to internationalize this problem. Once the United States started taking aggressive measures to reduce smoking domestically, tobacco companies started pursuing foreign markets and the U.S. government generally encouraged them. I could try to construct some “we’re all in it together” argument for why it would be bad to dump tons of prescription opioids on foreign countries, but it’s just immoral.
In terms of other ideas for cracking down on abuse, they get a bit fanciful in suggesting some political reforms that I think are not well-grounded in political science research or even necessarily constitutional. Certainly, though, we should all be a bit more skeptical of advocacy groups and industry lobbying.

The main problem here, really, is that we can’t really put the toothpaste back in the tube. There are some good ideas out there, like this John Kennedy bill to improve the safe disposal of excess prescription pills.
But we’ve already done a lot at this point to crack down on prescription drug abuse per se (sometimes with unintended consequences), and the problem now is that we have heroin and fentanyl markets all over the country. As they show, pill overdose deaths are actually gently declining, but that decrease is swamped by the rise in illicit synthetics.

There are obviously limits to the power of “just say ‘no’” messaging, but one does hope that word will get out that it is, in fact, a bad idea to become a heroin user. Past drug crises have proven to be somewhat self-limiting phenomena because addiction generates bad press for the product. But the slope on that curve makes waiting around for the problem to self-limit seem pretty scary. People thought the opioid problem was bad in 2015, and it’s become much worse.
Ideally, we’d increase the amount and quality of available treatment and make more of an effort to get people suffering from addiction headed in that direction rather than insisting on the dichotomy of going to prison or doing drugs on the streets.
Unfortunately, this is extremely difficult, both because treating drug addiction is hard and because of America’s tangled system of healthcare financing in which the insurance companies who’d foot the bill for treatment won’t necessarily reap the financial upside from effective treatment.
Medicaid finances a lot of drug treatment, though. Medicaid expansion also appears to reduce crime, and the main causal mechanism seems to be that Medicaid expansion increases the availability of substance abuse treatment. So it would be good for Texas, Florida, and the other holdout states to do the right thing and expand Medicaid.
But in keeping with the general hopelessness of this column, we do have to acknowledge that most states have expanded Medicaid, and the opioid crisis is still dire in a lot of those states. Indeed, most of the hardest-hit areas in Appalachia and the Northeast have expanded. So even though Medicaid is good, it’s clearly not good enough to halt the epidemic. We need a much bigger lever to change the treatment situation, and finding one that works is such a sufficiently large and complicated problem that it deserves an article of its own.
White women are still more likely to overdose than Black women, but the overdose rate for women as a whole is much lower.
"But even though the concentration in Appalachia does suggest some vaguely Case-Deaton-y conclusions, the rest of the regional pattern does not.... Maryland is the richest state in the union."
Gotta stop you there. You may be right that the opioid crisis is not primarily driven by poverty. But pointing to the wealth of Maryland is a total red herring. Maryland has extremes of wealth, and extremes of poverty. Maryland has Chevy Chase, and Maryland has Prince Georges County. And, famously, Maryland has Baltimore. They made a good tv show about it, once.
If you want to make your case about poverty not being a driver, then drill down to the county-level or finer. States like MD and CT have huge disparities of wealth within them. Talking about the wealth of the state as a whole is a disservice to your argument and to your readers.
My little brother died 2 weeks ago of a heroine overdose. Got started on oxy when he was 16 after an intense chest surgery. It was a decade of pain, struggle, lies, theft, rehab, false hope, and finally an end that none of us wanted but all knew was likely coming.
We come from an upper-middle class family in Houston, though my folks are now broke from all the rehab and we all had to chip in to pay for the cremation. I had my own struggles with addiction. Was an alcoholic for about a decade, though I was able to recover with the support of my immediate family and am 3 years sober. The dividing line between me and my little brother is very thin and blurry. We are separated only by a few simple decisions and a lot of luck. Common between us is that we were both ASD and both suffered from depression and anxiety before the introduction of any substances. I, eventually, learned how to manage and get my head over those, for the most part. He did not.