
We need to find ways to do faster clinical research
We have a new, faster way to test Covid-19 treatments — why doesn't the NIH use it?

The best study yet on the clinical effectiveness of ivermectin as a treatment for Covid-19 was released last week. The verdict? It doesn’t work.
The prior research wasn’t particularly promising, so this isn’t surprising. What is striking to me, though, is how long it took to get a high-quality study of a question that is obviously of great interest to a lot of people. And while there was no vast conspiracy on the part of Big Pharma to hide the truth, the normal model for conducting clinical research implicitly depends on Big Pharma envisioning a huge payday at the end of the process. If a company has bright shiny new mRNA technology with lots of patents, then they’re highly motivated to organize expensive trials and prove that those vaccines work.
But this isn’t the case with ivermectin, a widely available generic.
One of the companies that manufactures ivermectin could have paid for a study, but there would be no way for the company to internalize the benefits of its validation as a Covid-19 treatment. And since ivermectin was approved long ago as a safe and effective treatment for parasites, doctors are allowed to prescribe it for off-label use to Covid-19 patients.1 So nobody really stands to benefit from a rigorous ivermectin study, especially because rigorous evaluation might well prove that it doesn’t work.
And yet this seems like a question of vital public interest. If ivermectin did work, that would be very good to know. And conversely, given how many people talked themselves into believing that it does work, developing solid evidence that it doesn’t work is also valuable. Information in this sense is a classic public good: it’s not necessarily profitable to anyone to uncover better evidence about ivermectin, but it’s very good for society to have it. That’s exactly the kind of thing governments should fund. But they’re not.
Platform trials are delivering results
The ivermectin result itself was very widely covered in the mainstream news media, largely because ivermectin has become the subject of so much political controversy.
But the fact that ivermectin flunked a rigorous clinical trial was less interesting than the trial itself, which got less coverage.
The TOGETHER study has, for months now, been running large-scale trials on a bunch of medications already approved for other uses to try to find out if any of them can effectively treat Covid-19 patients. TOGETHER is how we know about the apparent efficacy of the antidepressant fluvoxamine as a Covid-19 treatment. And it was thanks to Kelsey Piper’s coverage of that finding that I learned about TOGETHER.
For the past year, [Edward] Mills has been using a new approach to clinical trials in order to test potential Covid-19 treatments faster. The key thing was to conduct them in parallel using what’s called an adaptive platform trial. “They’re multi-armed, so you’re testing lots of substances at a time, which allows you to only have one control group,” Mills told me. “What all of the useful trials in Covid have in common is that they’re an adaptive platform trial.”
Running, say, eight clinical trials, with eight control groups, requires many thousands of patients to get an informative sample, which can take a long time. Having eight experimental groups sharing a single control group cuts the number of patients required nearly in half.
This study model reallocates patients among treatment groups once a given treatment has been demonstrated not to work. That leads them to have larger, more convincing sample sizes for the most promising treatments. “You make decisions based on the data that emerges early,” Mills said. “After you have randomized 200 patients to the drug, if you can’t tell that it’s working, it’s probably not a very good drug. Every drug that’s not showing effects is a waste of patients.”
Matthew Herper at Stat used the ivermectin result as the peg for a piece on platform studies, writing “New Covid trial results may point toward better ways to study medicines” and explaining that TOGETHER was just one of several successful studies that all used a new and unconventional methodology.
TOGETHER, like the RECOVERY study conducted in the United Kingdom and REMAP-CAP, conducted basically everywhere but the United States, was a platform study, a streamlined clinical trial that evaluated multiple medicines at once and that use a common placebo group. It’s from these platform studies that doctors have learned perhaps the most about Covid-19.
One thing Herper notes is that these trials were “comparatively inexpensive,” with one costing $10 million and the other even less.
This kind of study isn’t appropriate for every question. And when a private company with a fancy new drug is eager to secure approval, there’s no problem getting them to shell out for traditional clinical trials. But researchers need a more cost-effective way to sift through a whole catalog of existing molecules, and platform studies are the only way to generate enough data per dollar to make that process worthwhile. This is why such a large share of useful information about Covid-19 treatments comes from this kind of study.
So you might think the NIH and other federal agencies focused on public health would be funding this stuff. But you’d be wrong. It’s all private donor money, mostly (according to Herper) from Stripe CEO Patrick Collison and FTX CEO Sam Bankman-Fried. It’s great to see these guys stepping up, but even really rich people like SBF (net worth $22 billion) and Collison (net worth $9.5 billion) have trivial amounts of money on hand compared to a major national budget.
Science has been underfunded during the pandemic
Unlike during the Great Recession, since March 2020 the U.S. government has forcefully deployed its fiscal resources in the face of emergency. The level of spending — $2.2 trillion in the CARES Act, $1.8 trillion in the American Rescue Plan, about $1 trillion in other smaller bills2 — has been huge, exceeding the post-9/11 military and homeland security surge.
But while the Great Recession was essentially a pure demand shock,3 the pandemic’s impact on the economy clearly has a lot to do with the real impact of the virus.
Illness has disrupted the economy, policies aimed at preventing the spread of illness have disrupted the economy, and individual efforts to avoid illness have disrupted the economy. So the biggest strides we’ve made in life-saving health interventions have also been our best economic interventions. That’s first and foremost vaccines, and increasingly (we hope) treatments like Paxlovid that should generate a massive reduction in mortality associated with breakthrough infections and illness in the unvaccinated.
Yet actual pandemic fighting has received remarkably scant resources amidst this emergency.
The hefty $1.8 trillion price tag for the American Rescue Plan apparently didn’t include enough funding for actual Covid-19 programs to last past this spring. The White House went back to Congress two weeks ago explaining that it urgently needed $20 billion to keep programs for vaccine administration, dispersing therapeutics, etc. going. Congress is going to cough up $10 billion, reducing the price tag in large part by zeroing out a request for $5 billion on global vaccination. That’s incredibly short-sighted, but it’s part of a larger pandemic politics trend where people yell at each other about masks rather than trying to address more fundamental issues.
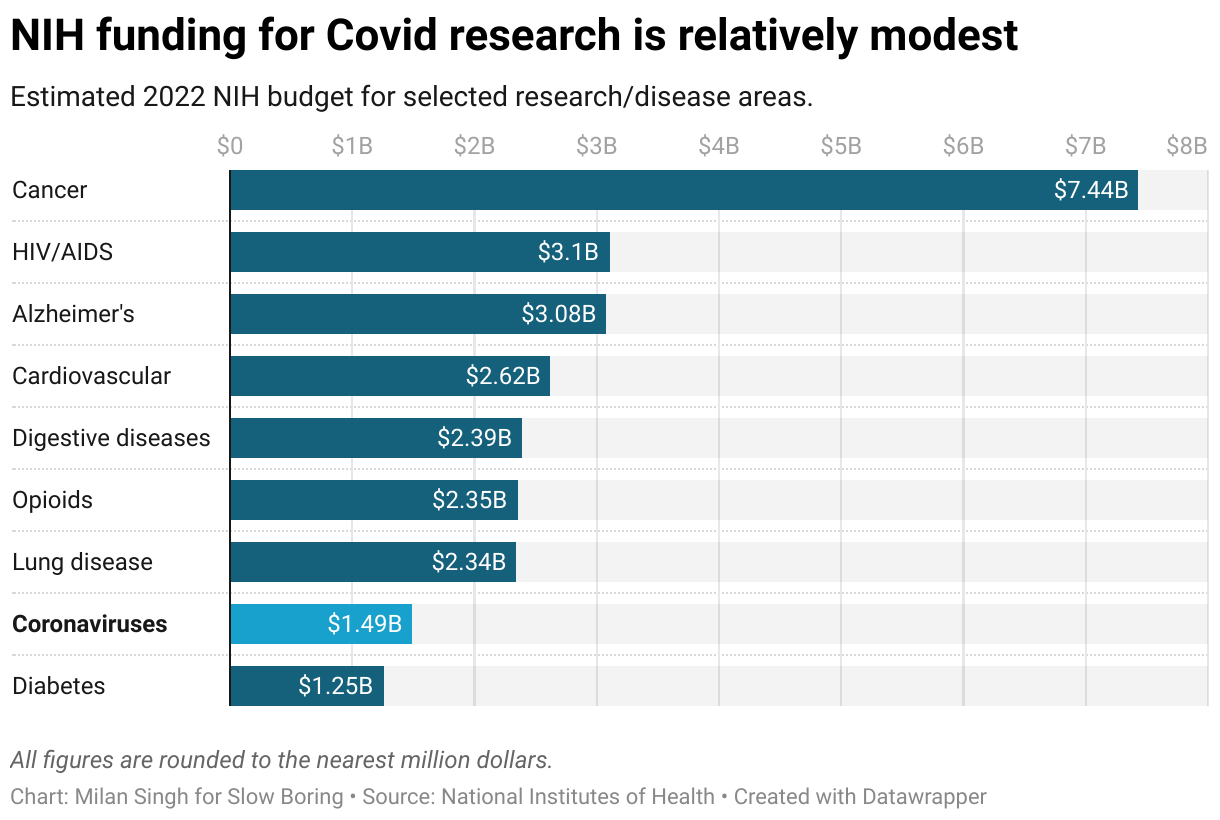
For example, while the NIH’s $2.5 billion in research funding on coronaviruses certainly should have been enough to spring for some of these platform studies, it just really isn’t all that much money. Eye disease got $1 billion. Neurodegenerative disease got $4 billion. A really big dog, like cancer, gets $7 billion. And cancer is obviously really important; it killed almost twice as many Americans last year as Covid-19. But it didn’t kill almost three times as many Americans. We’ve been researching cancer for a really long time at this point and have presumably picked a lot of the low-hanging research fruit. By contrast, with Covid-19, there are a lot of really basic, highly salient questions — like “does ivermectin work?” — that we’re only now sorting through. In 2022, the NIH estimated budget for coronaviruses is supposed to fall to $1.4 billion, less than for digestive diseases.
But I have a lot of questions.
I would like to know more about the novel coronavirus
I have a ton of questions about Covid-19 and ventilation that I think could be usefully answered with challenge trials — deliberately exposing rooms full of volunteers to the virus under different air filtering conditions to see how effective our different options here really are. I acknowledge that it’s considered unethical to let volunteers knowingly risk their personal health for the sake of the greater social good (unless you’re talking about a soldier or someone who cuts down trees for a living or dozens of other examples outside of the biomedical realm), and that’s a whole other article.
But in addition to scaling-up platform studies so that we can sift through more drug information, it would be great to see way more research focus on non-death aspects of the disease, including “Long Covid.”
Whenever I espouse skepticism about continued non-pharmaceutical interventions, I get a lot of “what about Long Covid?” in response. Honestly, I don’t think anything that we know about Long Covid meaningfully changes the cost-benefit math on mask rules or school procedures. But what we know about Long Covid absolutely merits a large investment in trying to understand what it is we’re dealing with and what treatments, if any, are effective. Like, this story about Welsh opera singers teaching breathing techniques to help Long Covid patients is interesting, but … does that really work?
Indeed, if you look at something basic like Jonathan Wolfe’s roundup of the state of knowledge about Long Covid for the New York Times, the state of knowledge is clearly really poor. Even a super-simple question like “do vaccines provide some protection against Long Covid?” has not been studied in a clear or rigorous way. Logically, it seems like there must be some protection since Long Covid is correlated (imperfectly, but correlated) with viral load and severity of symptoms, but it would be good to quantify the effect with a proper study design. We have these different variants; do they induce Long Covid to differing degrees? Maybe!
So how’s the research going? Well, according to Rachel Cohrs in a great March 31 piece for Stat, Congress agreed 15 months ago to provide the NIH with $1.2 billion to study Long Covid. That doesn’t strike me as a particularly massive sum of money given the scope of the issue, but it’s certainly enough to fund some good research. So far, though, we have zero clinical trials for Long Covid treatments:
But so far the NIH has brought in just 3% of the patients it plans to recruit.
Critics charge that the NIH’s missteps are even bigger: that it is acting without urgency, that it is taking on vague, open-ended research questions rather than testing out therapies or treatments, and that it is not being fully transparent with patient advocates and researchers.
This study “is a slow-moving glacier,” said Lauren Stiles, a former long Covid patient and a research assistant professor of neurology at the State University of New York at Stony Brook.“With a half-billion dollars, they could have run multiple clinical trials.”
It’s depressing.
Our institutions are failing and our politics is failing
I have a growing sense of despair about this. The U.S. government mustered trillions in pandemic relief funding but can’t scrape together $5 billion for global vaccinations or $60 billion to fund the White House’s own pandemic prevention proposal?
We’re under-investing in pandemic science and research, but at the same time, the government agencies whose job is to hand out the grants are so ossified that it’s hard to wish they had billions more to play with. And even though confidence in America’s public health institutions is eroding, there are no proposals in the works to actually reform them. On the Democratic side, people whisper complaints about the NIH or the FDA or the CDC lest they be seen as closet Trumpers. On the Republican side, the big idea is that we should throw Dr. Fauci in jail and I guess just not have public health research at all.
But nobody is willing to say the existing institutions are doing great and deserve to be pumped up with cash, nor are they willing to write legislation that would create new agencies or significantly reform the existing ones.
We’re just settling for institutions we’re not very confident in and not giving them very much money — then we sit around and hope for the best in terms of future variants or new pandemics.
Some of this really can be pinned on the institutions themselves or on small-minded politicians, but I also worry about the broader culture. My sense from years in the digital news game is that the big journalism brands are pretty good at giving people stories they want to click on, so if you want to stay on top of developments in areas like a pan-coronavirus vaccine or nasal vaccines that could actually block Covid-19 transmission, you find yourself in some pretty obscure publications. When politicians, pundits, or anyone else who wants an audience yells about something Covid-related, they yell about masks, not nasal vaccines.
I don’t want to paint too bleak a picture; the reason I am so convinced that our emphasis should be on biology and medical science is that we’ve seen some tremendous triumphs of biology and medical science. But this area needs much more focus and attention in terms of money, and most of all in terms of urgency, which ought to drive money but also flexibility and the creation of new institutions that don’t rely on a few eccentric billionaires.
To me, who likes things to make sense, this particular aspect of the American regulatory system makes no sense. If you want to sell a dietary supplement, you need to prove that it’s safe — there’s no need to demonstrate that it’s effective. But medication needs to meet the higher “safe and effective” standard to be approved. But then once it’s approved, it can be used even in cases where there’s no evidence of efficacy. But that’s a story for another day.
Annoyingly, the largest of these bills — the lame-duck Covid-19 relief bill that Mitch McConnell agreed to in a failed effort to win the Georgia Senate races — never acquired a fun name.
There was a real hiccup in the housing sector that was already causing the economy to slow in 2007 and early 2008, but it was no big deal until monetary policy errors and a banking panic destabilized demand in the fall of 2008.
You know what would go a long way towards answering a lot of these questions, like long covid and more? If everyone's medical records were kept in longitudinal consolidated databases, that can be aggregated, searched with algorithms to spot trends and correlations, etc.
Why don't we have that? In significant part because of overblown privacy fears that get the cost-benefit analysis wrong, loading up the cost side with vague, theoretical, hypothetical fears and dismissing likely concrete benefits.
The government is too hobbled and bureaucratic to get it done, though the recent interoperability rules for medical records are a big step towards making it possible for private companies to do it. Since the government can't/won't do this itself, it should get out of the way and focus on removing barriers and helping private companies do it responsibly, such insurance companies and vertically integrated IDNs. There's an enormous public health payoff if this can get done.
In the beginning of the pandemic, NIH issued a few NOSIs (Notice of Special Interest) for proposals on broad questions of SARS-CoV-2, including molecular biology and etiology. These dried up within a couple of months, even before their expiration as the small amount of money allocated was already spent. Now the only NOSIs are around downstream effects of COVID, messaging to underserved populations, and the like - nothing on biology or new treatments: https://grants.nih.gov/grants/guide/COVID-Related.cfm#active
In 2020, I submitted an R21 (two-year grant for exploratory research - $275k) to NIH on one of the SARS-CoV-2 proteins, for which we had a couple of publications already. It wasn't funded with the feedback being "there's already too many people working on this". Totally fair on the merits, but you might have thought in the first year of the pandemic that NIH would have wanted more people turning their research to SARS-CoV-2.
Talking to others, mine was a common experience. A collaborator had already developed a promising small-molecule inhibitor that not only worked in vitro against the virus, it even worked in a small humanized mice trial. They submitted an R01 (typical 5-year NIH research grant - ~$2m) proposal, which was not funded with typical stock criticisms.
Now, I don't want this to come off as a "woe is me" post; this isn't to say that my or my collaborator's proposals should have been funded no questions asked! But it's not just us. Having been on the other side of the equation, reviewing proposals for NIH in the last year, I can say there was no special attention paid to COVID-related proposals (if anything, it was more like an eye-roll at yet another one).
Maybe this is kind of self-serving, but it seems a bit tragic to me that after spending trillions of dollars to manage and mitigate the effects of COVID, we can't shake loose even a few billion for basic research.
Addendum: I have defended NIH before as the best way to decide what projects should be funded, and I still contend it's significantly better than the private grants that a lot of people are fond of. My complaint is that the high-level decision makers (e.g., Congress) didn't really prioritize SARS-CoV-2 research.