
Sure, don't "panic" about monkeypox — but it seems pretty bad
The situation has been getting worse for years and there's no sign of a turnaround

In Plato’s dialogue “Laches,” Socrates finds himself debating the meaning of courage with an important Greek general.
At first, Laches says that to be courageous is to be a soldier who holds his position in a phalanx in the face of danger rather than running away. Socrates replies that this seems very narrowly focused on infantry combat rather than on a broader question of character, which is important because earlier Laches argued that training young men for infantry service is good because it imparts the virtue of courage. If that’s to be non-circular, courage has to mean something more than simply correctly executing infantry tactics.
So Laches, in Jowett’s translation, replies that “courage is a sort of endurance of the soul.” Socrates then asks, “But what would you say of a foolish endurance? Is not that, on the other hand, to be regarded as evil and hurtful?”
Courage, after all, is a virtue whereas recklessness is not; endurance is only courageous when it’s wise. Scholars argue as to what Plato really means for readers to take away from this and even what genre of writing we should understand Laches to be. But I take his point as being about the interrelationship of facts and values.
And this is why I get nervous when sources as diverse as Science and the libertarian political magazine Reason are telling me not to panic about monkeypox.
Panic, after all, is the reverse of courage — it is by definition an inappropriate reaction to a dangerous situation. Sometimes standing and fighting is reckless, other times it’s courageous. Sometimes stockpiling groceries is panicking, other times it’s prudent. So it’s true that we shouldn’t panic in the face of monkeypox, but that’s simply because panicking is always a bad idea — that observation doesn’t tell us what we ought to do. And my sense is that the world is currently underreacting to monkeypox.
A stitch in time saves nine
People often say “don’t worry, it’ll be fine” about situations where the odds of “fine” are greater than the odds of “not fine.” But if you’re taking a road trip and Waze tells you that you could save 25 minutes by driving over a bridge that has a 10 percent chance of collapsing, you should not drive on that bridge. A person who says “don’t worry, it’ll be fine” and drives over the bridge for the sake of saving a little time is being reckless, not brave.
With regard to monkeypox, I’m happy to believe that the most likely outcome is that things will be fine. But the situation has been getting steadily worse over time, and the more humans who get infected with it, the more opportunities there are for mutations that will make the virus more transmissible or deadlier. Right now, monkeypox seems to spread overwhelmingly through skin-to-skin contact, which is relatively easy to prevent. But the WHO sees some evidence of spread through respiratory droplets. And we learned through the SARS-CoV-2 experience that there isn’t an incredibly hard-and-fast delineation between droplets and aerosols. What we know is that at the moment, monkeypox does not spread particularly efficiently.
That’s good. But rather than give us a sense of complacency, I think it should give us a sense of urgency. At the moment monkeypox is containable, so we should try really hard to contain it.
The monkeypox situation has been deteriorating for a while
To assess the severity of the current outbreak, it’s useful to look at the whole sweep of monkeypox history.
The virus was first identified in 1958 in lab monkeys, with several animal outbreaks throughout the 1960s. Scientists discovered that it was similar to the smallpox virus (variola) and also similar to cowpox virus and to the somewhat mysterious virus vaccinia that was cultivated by humans for smallpox vaccines.1 At the time, monkeypox wasn’t considered a big risk to human health because the smallpox vaccine was protective against monkeypox and the world was busy eradicating smallpox.
Then in 1970 we got the first human outbreak, as described in 1973 by Cheng Cho and Herbert Wenner:
Six human infections from MPV were reported in 1970 from the Democratic Republic of the Congo, Liberia, and Sierra Leone. All six patients were unvaccinated; each illness was diagnosed as smallpox based on clinical features of infection. The agents recovered from these patients were studied intensively by several reference laboratories and each was identified as MPV. The first case occurred in a 9-month-old infant residing in the Democratic Republic of the Congo. The four affected children in Bouduo, Liberia, ranged from 4 to 9 years of age. Three children who were playmates developed rashes on successive days, thus suggesting common exposure. The fourth child residing 12 miles distant from the others. The sixth case occurred in Sierra Leone; the patient, a 24-year-old male, had removed the stomach and intestines from a “red monkey” 3 to 4 weeks preceding onset of illness. None of the patients died of monkeypox. Moreoever, no other member of the households of these patients developed the disease.
Because these people were all unvaccinated against smallpox and also weren’t dying, the incident still didn’t generate major concern about monkeypox. The way to protect people from monkeypox was to give them smallpox vaccine, which the world was already doing. The main concern Cho and Wenner raised was that monkeypox might be seen as evidence that monkeys could contract smallpox, which would undermine the smallpox eradication campaign.
As for monkeypox itself, they found “no solid evidence for the transmission of MPV from person to person” but noted that this may be because so many people were vaccinated against smallpox. They concluded that “it appears advisable to protect persons against infection from such poxviruses by vaccination, especially those who handle monkeys.”
But within seven years of that article’s publication, smallpox was declared globally eradicated and children were no longer vaccinated against it. With more people unvaccinated, monkeypox began to spread. Several hundred cases were identified in the Democratic Republic of the Congo over the course of the 1980s with a reported case fatality rate of around 10 percent. As you can see in Nikola Sklenovska and Marc Van Ranst’s summary table from a 2018 article in “Frontiers of Public Health,” the situation in DRC deteriorated to the point where in the first decade of the 21st century, public health officials were no longer able to enumerate the cases and the disease had spread to the neighboring Republic of Congo. Then by last decade, a large number of cases appeared in Nigeria, with what seems to be a separate strain of the virus circulating there and in west Africa.

The world just didn’t respond to this. There was no mass mobilization to bring back vaccination campaigns in this part of the world. Rich countries treated this as an “out of sight, out of mind” African problem, so there was no emergency response — no money or equipment for monitoring mild or asymptomatic cases or for thorough genetic surveillance. And we didn’t really revisit the conclusion that human-to-human spread was unlikely, even though 1970s researchers said all along that was likely only due to widespread smallpox vaccination.
There was a small monkeypox outbreak in the United States in 2003 due to some imported rodents from West Africa. And a large, ongoing, and uncontained monkeypox outbreak happened in Nigeria over the course of 2018-2019, at which point the Covid-19 pandemic hit. Oyewale Tomori wrote in the summer of 2021 that “This year’s number is likely to be an under-representation because many people have been avoiding healthcare facilities for fear of contracting COVID-19 disease.”
Also in 2018, a case was detected in the UK when a person from Nigeria traveled abroad after developing an infection. Then in 2019, an English person went to Nigeria and brought monkeypox back. That same year, another traveler brought monkeypox to Singapore. Covid-19 reduced travel so the global spread stopped for a bit, but per Tomori’s point, the situation in Nigeria likely deteriorated. In May 2021, a traveler to Nigeria brought monkeypox back to Wales and infected other members of the household. Then in June, an American brought monkeypox back from Nigeria. The 2022 outbreak has been much more severe than any of these but, again, seems to have been originally linked to travel to Nigeria.
The point here is that throughout this whole history “monkeypox isn’t that big of a deal” has always been true, but it’s also been true that the situation has been continually worsening.
I recount all this history to contextualize reassurances that we can contain the current monkeypox outbreak with the point that we’ve been continually failing to contain it since at least the 1990s when it was clearly a growing problem in DRC. People have been warning that ignoring infectious disease problems in Africa and hoping for the best elsewhere would end up biting the whole world in the ass at some point, but that hasn’t stopped us from doing it (up to and including the pathetic efforts to provide Covid-19 vaccinations in Africa), so I think it’s good to worry.
We now have monkeypox superspreader events
Now one good piece of news we’ve gotten with monkeypox is that 10 percent case fatality rate in Central Africa does not appear to be indicative of the risk levels that we are dealing with. The strain present in Nigeria has lower reported lethality, but beyond that, the early CFR numbers tend to be overestimations, because people in desperately poor countries don’t go to the hospital to be checked for rare viruses unless they are seriously ill. So 10 percent of the people who were sick enough to go to the hospital died, but probably lots of people didn’t go to the hospital at all — and of course people in richer countries generally have access to better treatment.
It also continues to be the case that compared to a respiratory virus, monkeypox is relatively easy to contain. Spread happens most often due to prolonged close contact or direct touching of infected sores, and it seems like the virus spreads overwhelmingly when people are exhibiting symptoms. So in most case what you need is for health care workers to be very careful, for close family members to isolate, and since we have a vaccine available, we can use contact-tracing and ring vaccination to contain spread.
However, after making these points Keren Landman in Vox notes somewhat elliptically that there are conditions that could lead to super-spreading events:
While most lesions are painful, it might not be obvious to every infected person that they have monkeypox, especially early in the course of infection.
That is particularly salient in this outbreak, where many infected people have been reporting a rash localized to the genital area, often after close social or sexual contact. “Sometimes it’s dark, and you don’t inspect that very carefully,” [Vanderbilt University health policy professor William] Schaffner said, “so there are environments where transmission can occur, particularly if the contact is kind of semi-anonymous or fleeting.” In those scenarios, it might not be obvious to an infected person that they have symptoms and could be contagious. This concern could be mitigated with good public outreach (more on that below).
This isn’t incredibly common behavior, which is one reason that we’ve had endemic monkeypox in Nigeria for years without it spreading globally. But it seems like at least one person came down with monkeypox in West Africa and then went to either the Gran Canary gay pride festival or the Belgian fetish event Darklands or both.
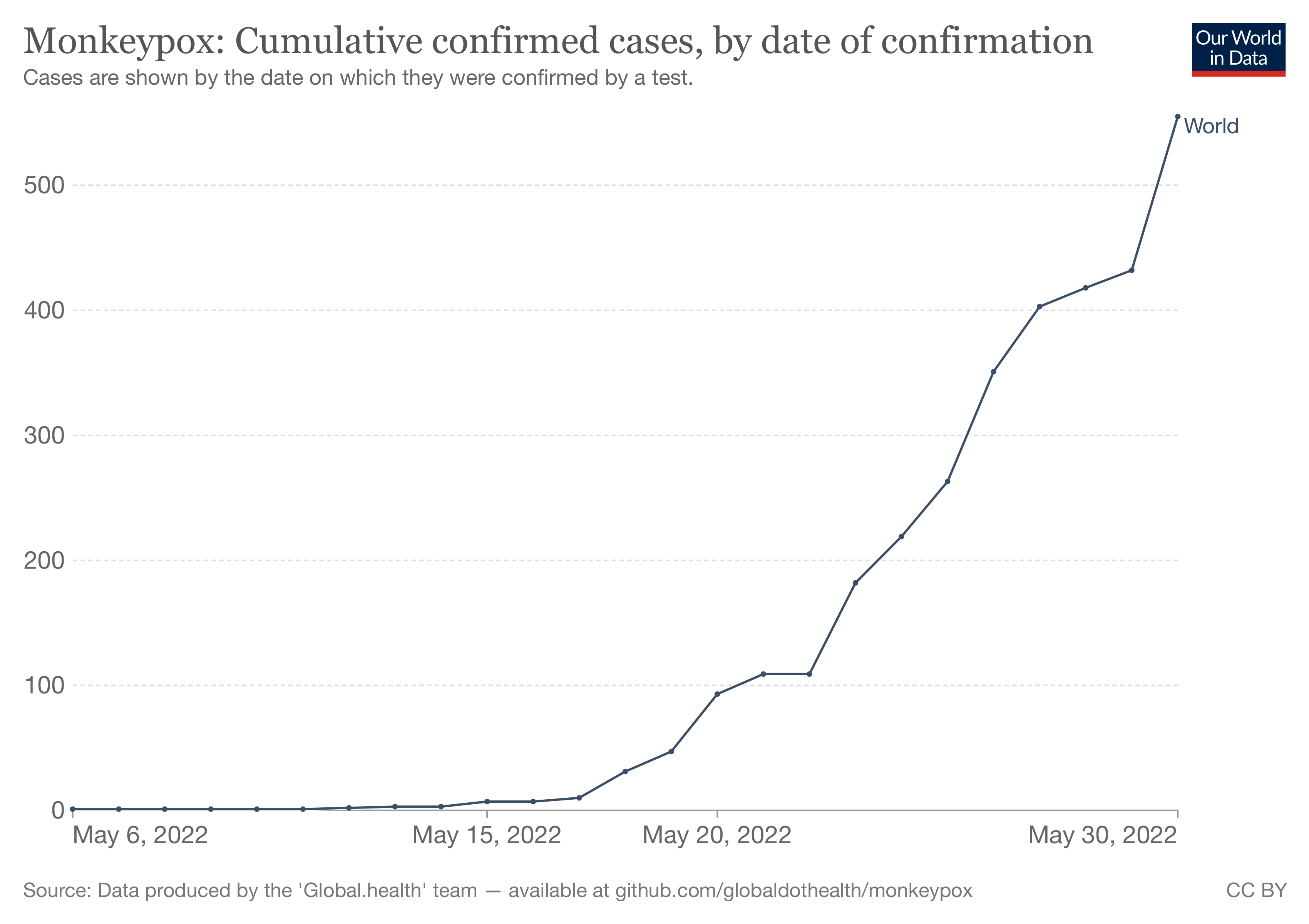
So we now have what I think is a problem that deserves to be taken more seriously as we head into June with big pride events in cities all around the world. The number of cases in the developed world is, as of yet, pretty small. But it’s popped up in many different countries and we don’t know of clear linkages between all the cases, so we know that undetected spread is happening. We also know from the global experience with HIV/AIDS that even if something starts circulating primarily among men who have sex with men, it has a decent chance of spilling over into other communities eventually.
Monkeypox right now does not spread efficiently enough to rapidly overrun the world’s hospitals, but it’s easy to imagine it spreading enough this summer to become endemically established around the world. And once it’s replicating in thousands of bodies in dozens of countries, the odds of mutations that increase virulence get scary. I don’t want to be too alarmist about this, but smallpox used to kill millions of people per year and eradicating it was one of humanity’s great triumphs. I think we really ought to be trying harder to prevent a new orthopoxvirus from becoming established.
What is to be done?
The first and most obvious thing is that we need to develop better capacity to test for monkeypox so it’s easier to tell what’s going on.
But as James Krellenstein, Joseph Osmundson and Keletso Makofane wrote recently in the New York Times, the current approach is like watching a replay of the Covid-19 testing fiasco:
Testing for monkeypox in the United States remains cumbersome. Currently, if a person is suspected to have monkeypox, their physician must contact a state or local public health department to test for the disease. Then, a C.D.C. laboratory partner runs a generic orthopoxvirus test on the sample. If that test is positive, the sample is sent to the C.D.C. headquarters in Atlanta so a monkeypox-specific test can be performed to confirm.
There are 66 public health labs that can test for orthopoxvirus. The C.D.C. estimates the partner labs have the capacity to test 6,500 orthopoxvirus tests per week, which the C.D.C. says is more than current demand. Between May 17 and 24, the labs were sent fewer than 60 samples for orthopoxvirus testing. Given that some of the cases detected so far appear to not be linked to travel, we remain concerned about efforts to identify and test ongoing community spread.
This is testing as a diagnostic tool to help doctors with their clinical practice. What we need is testing as a public health tool, which means that speed, cost, and ease of access are extremely important, even if that involves some compromise in accuracy, so that people who aren’t seriously sick can check their status.
We also need to think about vaccines. The smallpox vaccine that was used in the eradication campaign, Dryvax, unfortunately had a pretty nasty side effect profile. Smallpox itself was so bad that it was very worthwhile to run the campaign. Dryvax was replaced years ago by ACAM2000 which has never really been used in the general population and thus never got a brand name. ACAM2000 apparently has some virtues relative to Dryvax but a similar risk profile. The newest smallpox vaccine was licensed in 2019, and does have a name — JYNNEOS. It’s also new enough that it was marketed from the beginning as a dual-use smallpox/monkeypox vaccine. JYNNEOS has a much safer side effect profile2 and could therefore be more plausibly used against a less deadly disease like monkeypox. Unfortunately, JYNNEOS doses are pretty scarce at the moment. The CDC is releasing some of what’s already in the national stockpile and ordering more from the manufacturer, but also being pretty stingy in terms of who gets it.
My radical idea is to urge the public health community to drop its aversion to voluntary action and open up those ACAM2000 doses so they are neither required nor prohibited. We have a ton of these in stockpile, and my guess is that demand in practice is likely to be low, and the policy goal is to phase it out in favor of JYNNEOS anyway. Does everyone need to rush out and get a smallpox vaccination? No. If you’re a man who has sex with men and is planning to pursue a vigorous social life this summer, should you be given the option? I think so. The shots don’t help anyone in storage.
We should encourage vigilance, not non-panic
The good news about monkeypox — the reason not to panic — is that for most people, most of the time, “don’t accidentally touch another person’s skin lesions” is a pretty easy rule to follow. It’s much easier than “don’t accidentally breath air that contains invisible virus particles.” But if you do happen to lead a lifestyle that includes touching people the skin of people you don’t know well in darkened conditions, you might want to reconsider that at least temporarily. And if it’s important to you that you be able to do that, you might want to agitate for making the vaccine available so it’s safer.
For other people, there’s not that much we can do in practice at this point. But, again, rather than tell people who are concerned not to panic, we should be as vigilant as is reasonably possible — learning what the symptoms look like and other good, factual information so you can be an asset to your social circle in terms of information.
In terms of policy, the fact that we’re not where we should be in terms of tests or vaccine manufacturing capacity is a reminder, once again, that we could desperately use more focus on pandemic prevention. Any given zoonotic virus probably won’t cause the level of damage of SARS-CoV-2. But SARS-CoV-2 was very damaging. And worse things could come around the bend. Monkeypox probably won’t be that worse thing (you don’t need to panic!) but it could be, and even if it ends up being fine, none of the climate shifts and habitat stresses that generate virus crossovers are going away. We need to work on this stuff with much more urgency.
Edward Jenner, famously, showed that you could inoculate people against smallpox by deliberately infecting them with cowpox. It seems he also thought that cowpox and horsepox were the same thing when we now know they are distinct viruses. Nineteenth-century doctors took Jenner’s insight and started cultivating what was either cowpox or horsepox or both (often in sheep) for vaccination purposes without keeping very clear records. By the time 20th century genetic analysis was possible, it was clear the virus used for vaccination purposes was quite distinct from naturally occurring cowpox or horsepox — genetic engineering had created a new virus.
Part of that is that even though it also uses live vaccinia virus, it has been disabled. How? Ask a virologist! Something called “serial passage” is involved as I understand it.
At least this one has a scary name and gross effects.
Sometimes it’s the little things that get people to act more rationally.
I won't repeat the gravest sin of the public health establishment and those in their circles: I won't tell a well-meaning lie to try to coax the behavior I want.
I will tell them the truth: they are operating at a severe credibility deficit, and I am *very* reluctant to say a version of "I will let the CDC tell me when I can stop paying close attention to issues that people at the CDC personally think are important".
I just can't muster it right now. I think most can't. I hope the establishment attempts to engage the population where it is rather than where it wishes we were, but lol.