
End the Medicare For All wars
It's time to talk about other health care policy ideas

I’m a little uncomfortable with the fact that health care policy is back on the American political agenda because of the murder of UnitedHealth Care’s CEO. But, given that it is, I do want to write about it.
But first, I want to write about something more meta.
The murder has people talking about health care policy, in particular about health insurance companies. The question of how much to villainize these companies is very much a matter of debate within the American left-of-center camp (recent articles from Noah Smith and Eric Levitz fall on the anti-anti-insurer side of the argument). But taking a step back, I think it’s worth noting that the subtext to this debate is about Medicare For All and thus, to some extent, about the 2016 primary. Because really, every conversation about health policy in the United States becomes almost immediately about Medicare For All and about the 2016 Democratic Party primary.
When Bernie Sanders’s campaign manager Faiz Shakir was on Ezra Klein’s podcast recently, he casually mentioned that had Sanders become president in 2017 or 2021, there wouldn’t have been a Medicare For All bill. Here’s what he told Ezra:
One of the things that you know about him and I know is that there’s a high degree of pragmatism there.
So while he’s pushing, let’s take Medicare for All. Then he gets into Congress: And can we at least lower the age from 65 to 60? Can we talk about Medicare expansion so that it covers home care, dental, hearing and vision — even if you can’t all move with me to Medicare for all? That actually is how we’re President Bernie Sanders would have governed.
This is also what I think would have happened, and it means that all the pixels that have been spilled over the past decade on Medicare for All are essentially pointless.
Bernie is not the first politician to toss out chum for the sake of a primary campaign, and he won’t be the last. But the unfortunate legacy of the 2016 primary is that everyone took their positions a little too seriously. Sanders fans emerged from the experience claiming that any outcome short of Medicare for All would be an unacceptable betrayal, when in fact, any president would find themselves working with Congress to try to pass some incremental health care reforms. Bernie sometimes plays fanatic on the internet, but he’s actually a veteran member of Congress who knows the score.
And now that he’s not running for president anymore, I think it’s time for a serious conversation about the kinds of incremental proposals Democrats should prioritize.
Setting priorities is important
I don’t think it would have made a difference whether the president-elect ran on a platform of Medicare for All (Sanders) or a public option (Biden) or on Medicare For All Who Want It (Buttigieg).
The difference comes down to two things:
How many Democrats win seats in Congress?
Once they take power, what is the priority of the administration, the thing that it begs moderate members to help on, while promising to cut them slack elsewhere?
Republicans, I think, do a good job of synthesizing the kind of visionary approach that Shakir advocates for with the brass tacks awareness of (1) and (2). Every cycle, a GOP presidential candidate runs on a bunch of ambitious, confusing, somewhat vague tax pledges. Then Republicans up and down the ballot mostly run by talking about cultural wedge issues, with nobody attacking frontline members from the right for failing to publicly affirm sufficiently extreme positions. And every time Republicans win, they prioritize enacting some large tax cut, the specifics of which get worked out in Congress based on the numbers.
This all really just means that the prospects of health care reform come down to prioritization squared.
On the one hand, and related to (1) above, I think Democrats should make expanding access to affordable health care closer to the core of candidate recruitment. Some parts of the country have very restrictionist sentiments about immigration. Some parts of the country are very enthusiastic about the second amendment. Some parts of the country feature a majority composed of non-college white people who don’t want to be lectured about how privileged they are. Every part of the country has some important local business interests that voters want protected. But all across the country, Democrats are fundamentally more trusted on health care issues, and voters are sympathetic to the idea of government activism to get more people the treatment they need. That’s why Medicaid expansion can win in states like Kentucky and West Virginia. But Democrats need to prioritize this issue in their red state recruiting, which means allowing for moderation on other issues, not just asserting that the cultural divide can be evaded.
Then, on the other hand, Democrats need to actually prioritize health care in office, or point (2) above.
By November 2020, it was clear that, despite the Medicare For All debates, the Democratic Party had decided to prioritize climate policy.
I think it’s important to acknowledge that this was a party-wide call that transcended factions. Joe Biden chose to prioritize climate issues when defining what it would mean to “build back better,” and to the extent that he took heat from the left, it was over concern that the Bipartisan Infrastructure Law wasn’t prioritizing climate enough. The reason the 117th Congress made only relatively minor changes to health care policy isn’t that Biden didn’t run on sufficiently visionary health care changes, it’s that the party as a whole emphasized a different policy topic. I don’t know whether a Sanders administration or a Buttigieg administration or a Klobuchar administration would have made a different choice. My suspicion is that they would not have, that despite putative tensions between leftists and the establishment donor class, both sides actually viewed climate as the most important issue. But it’s unknowable.
Prioritizing health policy doesn’t mean giving up on climate policy. But it does mean checking the influence of environmental groups and adopting an abundance-oriented approach that can secure bipartisan support. I’ve heard a lot of positive things about Arnab Datta’s op-ed on this from influential Democrats in the climate space. But what’s not clear is whether they’re talking about an abundance-oriented approach as a necessary evil after an election loss, or as an ethic to carry forward into the future.
It’s just not possible to build an electoral coalition for changing health care in a serious way if you insist on picking hyper-partisan fights about energy. Democrats can certainly make some progress on both topics in a partisan way (Biden did), but there are limits and tradeoffs.
What do we want to do?
Going back to Faiz’s conversation with Ezra, I want to flag that “lower the Medicare age to 60” is more different from “Medicare for All” than it might sound.
That’s because “Medicare,” the actually-existing federal program for senior citizens, has wildly different characteristics than the “Medicare” in Medicare for All. Medicare, as Shakir mentions there, doesn’t cover dental, hearing, or vision. Medicare has premiums and copays. Medicare has a robust private option called Medicare Advantage. Even lowering the Medicare eligibility age to zero, ensuring all Americans are on Medicare as it currently exists, would fall far short of the Sanders Medicare for All proposal.
That’s why another example of incremental change that Shakir mentions is adding dental, hearing, and vision coverage to Medicare.
Which is to say that you can think of proposals as existing on two separate axes, one of which is expanding existing programs.
Sanders wants to make the coverage provided by public programs (notably Medicare) more robust, and he wants to expand the number of people who are covered by the public programs. These are both reasonable goals (though personally, I would say expanding the number of people covered is more morally urgent than making the coverage package more generous).
I would also say that in general, I don’t love the idea of focusing incremental expansions on the oldest Americans. A big problem in the politics of health care is that while elderly people love their Medicare, this doesn’t make them want to extend the program to other people. Instead, they take an “I’ve got mine” attitude and seem to worry that further expansions of insurance coverage will compromise their care.
My preferred version of “make existing public programs better” is to improve Medicaid (which currently has very low reimbursement rates and thus many providers refuse to accept it) by integrating it better with Medicare. And my preferred version of “get more people on the program” is something like Medicare For All Kids. My feeling is that if children are enrolled in a public program and they and their parents like it, that could build political momentum for expanding the program so they don’t get kicked off.
Cost and supply
Beyond coverage, there’s a whole other axis related to costs.
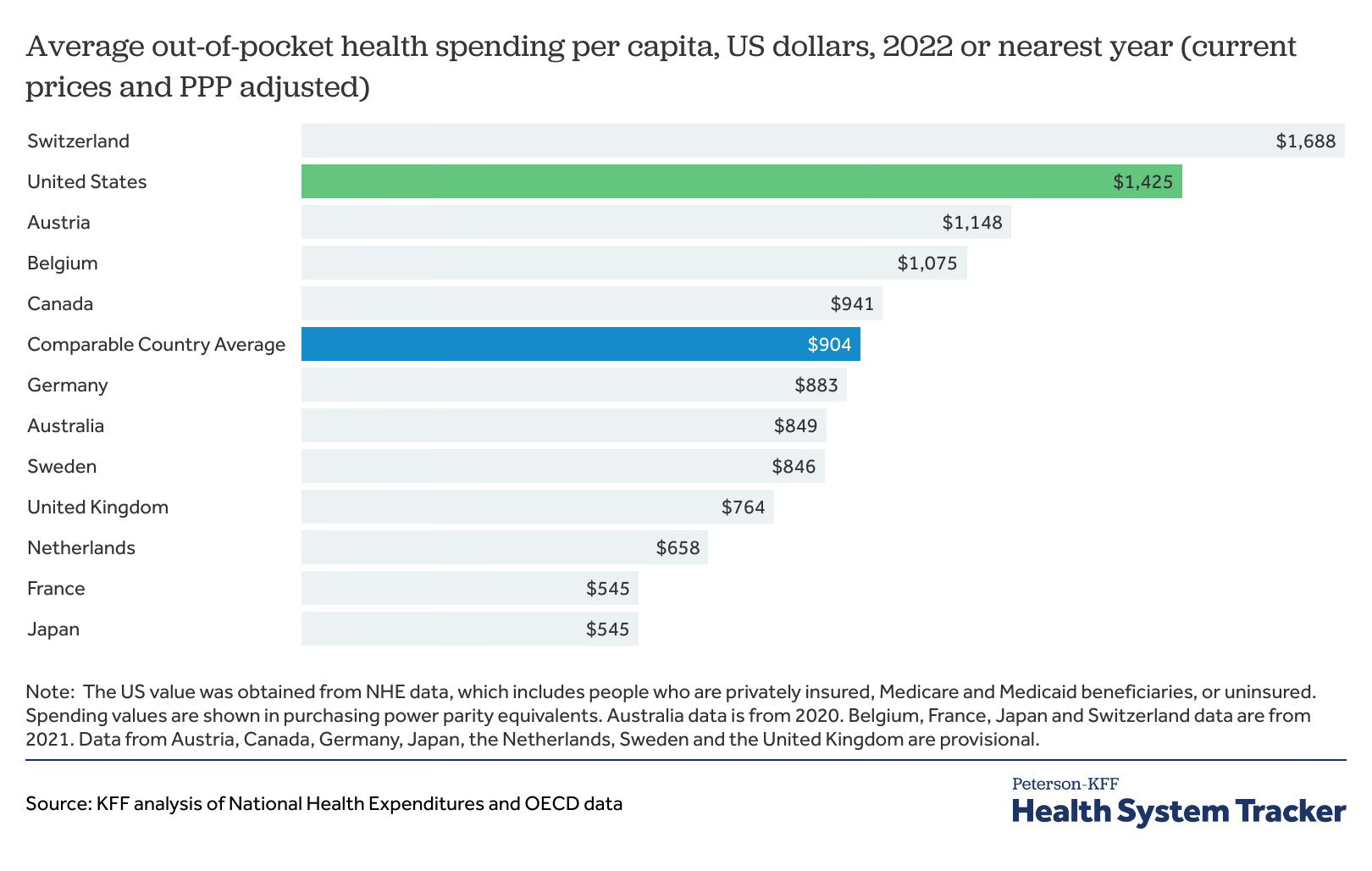
Despite sometimes spotty insurance coverage, Americans actually have an unusually low share of out of pocket costs compared to people in many other comparable countries.
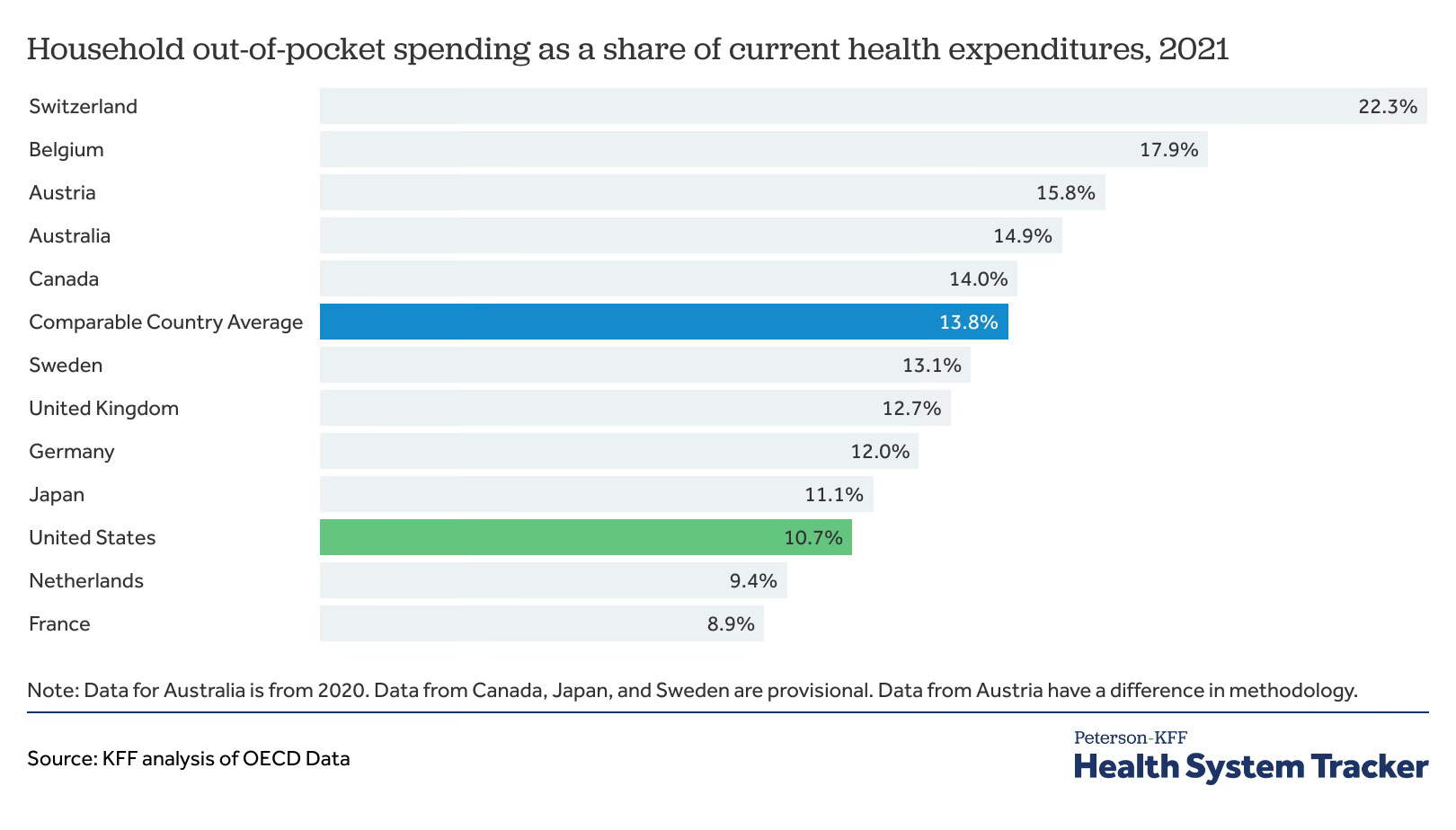
The bad news is that we’re paying more anyway because the prices are higher across the board.
Some of this is just straight-up price controls. Even Singapore, which conservatives often praise as a system with many market-driven features, has a de facto system of price controls that it characterizes as benchmarks.
But there’s also just a lot of genuine waste in the American health care sector. There was no such thing as an airplane industry until people figured out how to make airplanes that worked. People tinkered with heavier than air flight for a while, but nobody made money off of it until the technology functioned. Health care isn’t like that. The medical profession has existed for much longer than there’s been any actual medical science. Those who are ailing will gladly pay money for things that don’t actually work. Many people are interested in getting tests that aren’t well-supported by evidence or statistics. David Cutler says that “between one-quarter and one-half of medical spending is not associated with improved health.”
And note that’s a pretty low bar. Some medical spending that is associated with improved health still isn’t going to pass a reasonable cost-benefit bar. People will sometimes get into arguments on the internet about “the real problem” in American health care, but the truth is that health care is a very large swathe of the economy and it features multiple problems. We have examples of people bankrupted due to lack of adequate insurance, we have examples of people deferring or avoiding useful care due to financial precarity, and we also appear to have lots of spending on things that have little-to-no actual value.
But not only is the food bad, the portions are often too small. As Lawson Mansell writes, in recent years we’ve seen an incredible amount of pure price inflation in physician services and hospital bills.

Some of this is due to anti-competitive consolidation, where small-scale mergers have generated a lot of localized monopoly power. A lot of it is barriers to entry — limits on the training of new physicians, on the ability of immigrant doctors to practice, and Certificate of Need laws that block the creation of new health facilities and prevent adequate supply of health care services. This entire thicket of topics is a little more conceptually complicated than the parallel issues around housing, since there are valid reasons for regulating who can market themselves as a health care provider, and the question of health care waste has no real parallel in the housing space.
But this is all just to say that health policy is multi-faceted and doesn’t need to be tackled all at once.
There are things we can do to improve access. There are things we can do to reduce waste. And there are things we can do to improve supply. It doesn’t need to be a single big bang reform. Shakir’s concession that it was all going to be incremental changes anyway means we need to stop having all-or-nothing health reform conversations. We should also recall that foreign countries, whatever their health care system, don’t just have an end to politics. Canada, France, the UK and every other country have constant political disputes about health care funding levels and exactly how things should work. Politics isn’t going away. What we need is to put specific ideas on the table, debate their merits, and try to pick priorities.
This article is a breath of fresh air that I'm glad is now on the record at SB. It's long been exhausting to listen to broad, vague, pie in the sky demands for universal healthcare, without covering sufficient details as to how it's going to happen given the current facts on the ground.
Obviously, as this is coming from me, the rent seeking much be attacked, including via the avenues Matt listed. Steadily expanding the fringes of public coverage is also sensible. A public option to opt into would be more ambitious but I think doable if that ambition starts off limited. Bore slowly, but nonetheless bore.
I’m genuinely just constantly surprised how fucking stupid people are talking about healthcare policy.
Like the number of my friends who will confidently assert that every other country in the world has a model like the UK or Canada’s is just mind blowing. And if I mention to them something like all payer rate setting as a key piece of most countries healthcare it’s like I’m speaking some weird language. Like all the technocratic stuff you get from reading health reporters is just uninteresting.
What’s especially frustrating is several of the most Sanders’s pilled people I know I met as an English teacher in Korea and thought the system was wonderful . Which I don’t fully understand all the details of but it’s not like that at all.